 Mosquito used to illustrate the story.
Mosquito used to illustrate the story.
Malaria continues to be a major public health problem in 97 countries and territories in the tropics and subtropics.
Globally, approximately 214 million cases of malaria occur annually and 3.3 billion people in 106 countries are at risk of being infected. Approximately 438,000 deaths were attributed to malaria alone in 2015, particularly in Sub-Saharan Africa, where an estimated 90 per cent of all malaria deaths occur.
As a critical target of the Millennium Development Goals, in 2005, the World Health Assembly established a goal of reducing malaria cases and deaths by 75 per cent between 2005 and 2015.
Hence, over the past decade, there has been renewed interest in research and innovations in diagnostic methods, drugs and vaccines, and the development of control measures to eradicate malaria.
As a result, between 2000 and 2013, the incidence rates of malaria fell by 30 per cent globally, and by 34 per cent in Africa.
Malaria is one the endemic disease which has killed 400,000 babies and claimed so many pregnant women lives
In Nigeria
Nigeria suffers the world’s greatest malaria burden, with approximately 51 million cases and 207,000 deaths reported annually (approximately 30 per cent of the total malaria burden in Africa), while 97 per cent of the total population (approximately 173 million) is at risk of infection.
Moreover, malaria accounts for 60 per cent of outpatient visits to hospitals and led to approximately 11 per cent maternal mortality and 30 per cent child mortality, especially among children less than five years.
Malaria is caused by Plasmodium falciparum, and the mosquitoes Anopheles gambiae, Anopheles funestus, Anopheles arabiensis, and Anopheles moucheti are the major vectors that cause year-round transmission. Artemether-lumefantrine (AL) or artesunate + amodiaquine (AS + AQ) is the treatment regime adopted in 2004.
This devastating disease affects the country’s economic productivity, resulting in an estimated monetary loss of approximately N132 billion (~700 million USD), in treatment costs, prevention, and other indirect costs.
Since 2008, the National Malaria Control Programme (NMCP) in Nigeria has adopted a specific plan, the goal of which is to reduce 50 per cent of the malaria burden by 2013 by achieving at least 80 per cent coverage of long-lasting impregnated mosquito nets (LLINs), together with other measures, such as 20 per cent of houses in targeted areas receiving indoor residual spraying (IRS), and treatment with two doses of intermittent preventative therapy (IPT) for pregnant women who visit antenatal care clinics.
Due to these measures, the percentage of households with at least one LLIN increased to over 70 per cent by 2010, compared to only 5 per cent in 2008.
Level of coverage still a huge challenge
However, the way a country finances its health care system is a critical determinant for reaching Universal Health Coverage (UHC).
This is so because it determines whether the health services that are available are affordable to those that need them. In Nigeria, the health sector is financed through different sources and mechanisms.
The difference in the proportionate contribution from these stated sources determine the extent to which such health sector will go in achieving successful health care financing system. Unfortunately, in Nigeria, achieving the correct blend of these sources remains a challenge.
As Nigeria celebrates the World Malaria Day 2018, with the theme “Ready to beat malaria” the coverage of malaria in Nigeria is still far behind.
World Malaria Day is an international observance commemorated every year on April 25 and recognises global efforts to control malaria.
Nigeria has 34,173 health facilities nationwide which include 30,098 primary health centres, 3,992 secondary facilities, and 83 tertiary facilities. The private sector constitute 33 per cent of all facilities in Nigeria, yet there is still a hole in our malaria coverage
Huge funds deployed over the years
Nigeria has benefited from support from various international donor partners for malaria control, over the years past. Currently, the largest funding partners includes, the Global Fund, the U.S. Government, and United Kingdom Department for International Development (DfID).
Also, other key partners include the United Nations Children’s Fund (UNICEF) and the WHO. There are also other corporate private sector support for malaria control including ExxonMobil, Chevron, Royal Dutch Shell, Dangote Foundation, and telecommunication companies. The Global Business Coalition through the Corporate Alliance on Malaria in Africa is galvanising corporate efforts to support resource mobilisation as well as to leverage the strength of this sector.

The World headquarters of the World Health Organization (WHO) in Geneva
[Photo Credit: VOANEWS]
In 2014, Nigeria had three approved grants for malaria from the Global Fund, the latter two designating the NMEP as the Principal Recipient. In March 2015 the country and the Global Fund signed the New Funding Model (NFM) grant totaling to over $400 million for two years.
The approved grant for Nigeria under the NFM was $400,253,346 to cover the period of February 2015 to December 31, 2016. The fund was managed by the NMEP ($308,577,343) and the Society for Family Health ($91,676,003) as Principal Recipients.
As of the end of January 2016, $279,554,526 was committed to support various malaria activities, including procurement of malaria commodities. The Global Fund included a requirement that the Nigeria Government to provide $22.5 million as counterpart financing for ITNs; however, the counterpart finance is yet to be provided.
The current Global Fund agreement, signed in 2014, originally required the Nigerian Government to provide $45.7 million in counterpart funding for net distribution. When the Government failed to provide those funds, during grant extension negotiations in 2017, the Global Fund agreed to halve the amount required to $22.5 million.
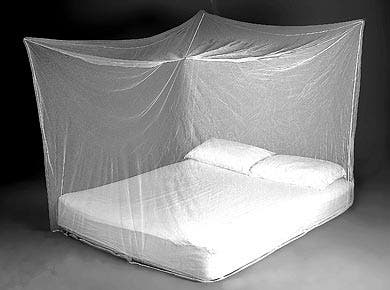
Insecticide treated mosquito nets that helps prevent malaria, being displayed.
To date, the government has not provided this amount. The current Global Fund grant ended in December 2017, and unless Nigeria government funds are provided prior to that grant expiration, counterpart funding requirements will not have been met.
As of April, 2017, a non-costed extension was granted for the Nigeria malaria grant, as well as a one-year grant with a new Principal Recipient, Catholic Relief Services, to implement long-lasting insecticidal net (LLIN) replacement mass campaigns in six states and continue implementation of the other malaria program activities through December, 2017.
The extension and one-year CRS grant will maintain the scope and scale of essential malaria services in 2017 and will be funded through reinvestment of unspent funds within the current grant.
In terms of activities, the Global Fund grant supports scale-up of prevention and case management activities in line with the NMSP 2014-2020. The key interventions are to attain universal coverage of ITNs through mass campaigns and continuous distribution channels.
About 10 states were included in the project and Kogi, with a prevalence of malaria in children of under five years of age of 5 per cent, was replaced with Plateau State with the parasite in children under five years of age of 36 per cent. Support to Kogi State was phased out in 2017. The projected population of the 11 states to receive PMI (President’s Malaria Initiative) support in 2019 is 57.8 million.
The PMI is a U.S. Government initiative designed to cut malaria deaths in half in target countries in sub-Saharan Africa. It was announced on June 30, 2005, when President Bush pledged to increase U.S. funding of malaria prevention and treatment in sub-Saharan Africa by more than $1.2 billion over 5 years (FY2006-FY2010).
A recent additional resource for the states is the Saving One Million Lives Initiative (SOML) Program-for-Results (PforR) Project. The objective of this US$500 million World Bank-funded project is to increase the utilisation and quality of high impact reproductive, child health, and nutrition interventions. Still, external funding does not cover all technical assistance and implementation support needs for all health facilities within these 11 states.
The World Bank
Roll Back Malaria
Roll Back Malaria (RBM) Partnership was launched in 1998 by the World Health Organization (WHO), the United Nations Children’s Fund (UNICEF), the United Nations Development Program (UNDP) and the World Bank.
Its goal was to provide a coordinated global approach to fighting malaria.The RBM Partnership is the global framework for implementing coordinated action against malaria. It mobilises resources for action and forges consensus among partners.
The Partnership is made up of more than 500 partners, including countries where malaria is endemic, their bilateral and multilateral development partners, the private sector, nongovernmental and community-based organizations, foundations, and research and academic institutions. The Global Malaria Action Plan defines two stages of malaria control: first, scaling-up for impact (SUFI) of preventive and therapeutic interventions, and then sustaining control over time.
Coverage and Implementation
Nigeria began implementation of Presidential Malaria Initiative (PMI) in the fiscal year (FY) 2011. PMI began with support to three states (Cross River, Nasarawa, and Zamfara).
In 2012, PMI expanded to six more states (Bauchi, Benue, Ebonyi, Kogi, Oyo, and Sokoto), and in 2013, added two more states (Akwa Ibom and Kebbi) for a total of 11 states.
A strategy review meeting held in April 2016 revisited the states for PMI support. States were selected based on malaria disease burden, coverage, presence of other donors, strength of state leadership, and security.
In 2016 2.7 billion US dollars was invested in malaria control and elimination, 74 per cent of the investment in 2016 was invested in some countries in Africa which are endemic of the disease larger percentage goes to the Sub-Sahara Africa where Nigeria is at the frontline.
Data shows that 76 per cent Nigerians lives in high transmission areas and 24 per cent in low transmission areas.
The Nigeria Malaria Indicator Survey of 2014-2020 objective is to achieve universal coverage with Insecticide Treated Net (ITN).
Universal coverage on malaria elimination is defined as one ITN for every two persons. PMI’s goal is to support the NMEP in achieving and maintaining its targets for ITN coverage and use, especially in PMI-supported states.
PMI supports free mass ITN campaigns every three years and strengthening continuous distribution channels that include antenatal care (ANC) and immunisation clinics, schools, and community-based distributions where feasible and cost-effective.
Since 2010, PMI has procured a total of 40.7 million ITNs for mass campaigns and continuous distribution, and distributed over 60 million ITNs, including over 24 million ITNs procured by other partners. From December 2013 to May 2017, the NMEP and its partners says it distributed 60.8 million ITNs through mass campaigns in 23 states, including over 26 million ITNs in all the 11 PMI-supported states of Sokoto, Bauchi, Nasarawa, Kebbi, Cross River, Ebonyi, Zamfara, Benue, Akwa Ibom, Oyo and Kogi.
Data from two Nigeria Malaria Indicator Surveys (NMIS) show ownership of at least one ITN in a household increased substantially from 8 per cent in 2010 to 69 per cent nationally in 2015. The average number of ITNs per household doubled from 0.8 to 1.6 (2015 NMIS). Eight of the 11 PMI supported states had higher ownership of at least one ITN per household than the national average.
An expert speaks
Ladipo Olabode Taiwo, a public health practioner scores the Federal Govenrment low on disbursement of funds to tackle the ailment and also on accurate data gathering on it.
“There has not been any concise figure/amount released by Nigerian government for the funding of malaria elimination in the country,” he said.
He also explained that the states that are not under the PMI coverage for malaria are taken care of by Global Fund.
He spoke about the “poor health financing been practiced by the Nigerian Government”.
“If not for PMI, Global fund and other NGOs who have supported the country in the health sector, the country health sector would be nothing to talk about.
He said malaria data collection in Nigeria is not 100 per cent accurate, or “representative of what is happening”.
“The reason is that most of the data are collect at the ‘lower level’, and the states has just 24 hours to check the data and validate them, and most states do not have a data bank with the Federal Ministry of Health.”

Isaac Adewole, Minister of Health.
He however said there is a decline in the cases of malaria in Nigeria, “as a result of the management which was set up by the National Malaria Elimination Program’’.
‘‘The year world malaria day is an avenue to orientate and educate the citizens that malaria is curable and preventable, so that every body will be ready to beat malaria,” Mr Taiwo added.
